



By Prof. Dr. J. M. Hans, Padmashree Awardee, Senior Consultant, ENT Specialist
Madhukar Rainbow Children’s Hospital, Malviya Nagar, New Delhi
Tonsil cancer is the most common type of oropharyngeal malignancy, comprising 23.1% of all malignancies in this region. There has been a sharp rise in its incidence in the last many years due to the increase in HPV-induced cancers. The “viral epidemic” of HPV had dramatically increased the incidence of oropharyngeal cancers in the last 40 years.
CAUSES (ETIOLOGY)
We have blamed smoking and alcohol misuse for causing tonsil cancer traditionally. Smoking is a poor prognostic factor independently. However, in recent years, cases secondary to HPV have increased highly. HPV-16 is the most common strain found in oropharyngeal cancers. Traditionally, in addition to smoking and spirits, sharp tooth, spices, syphilis, and sepsis have also been attributed to oropharyngeal cancer.
RECENT UNDERSTANDING OF HISTOPATHOLOGY
Tonsil cancer is a squamous cell carcinoma. WHO distinguishes tonsillar SCC into HPV-positive and HPV-negative types. HPV-positive SCCs have a non-keratinizing morphology and arise from the deep lymphoid tissue of the tonsillar crypts. HPV-negative SCCs arise from the tonsillar surface epithelium and show keratinizing dysplasia. P16 is a tumor suppressor protein over-expressed in HPV-positive tumors and is an important marker.
SYMPTOMS AND PRESENTATION
Generally, HPV-positive tumors are seen in young non-smoker people of either gender whereas HPV-negative tumors are seen in older males who smoke and have other co-morbidities. The latter has a poorer prognosis.
Some of the common presentations are:
- Sore throat
- Unilateral otalgia
- Sense of fullness in the throat
- Trismus (if there is local invasion)
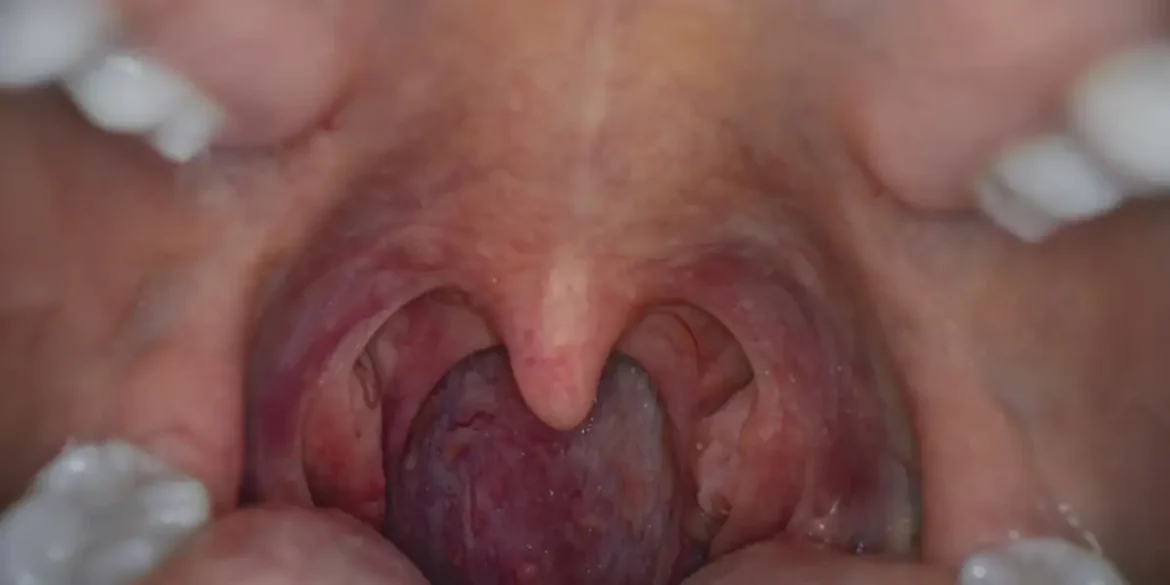
- Asymptomatic patient with an incidental finding of asymmetric tonsils
- Occult lesion with enlarged neck nodes (JD nodes)
We must always keep in mind the following symptoms – weight loss, loss of appetite, hoarseness of voice that’s persistent, and difficulty or pain while swallowing. A full ENT examination along with palpation of the neck is ideal. The tongue base, vallecula, lateral pharyngeal wall, and post-nasal space must also be examined.
EVALUATION AND TESTS
A pan-endoscopy is done to rule out secondaries and skip lesions in the upper airways and esophagus. It helps plan surgical management. Radiological investigations include MRI, CT, and PET-CT. MRI with contrast helps delineate local spread and gives the best views of soft tissue. CT skull base to mediastinum gives us details about the primary tumor as well as any lung or nodal disease. PET-CT can be used in difficult-to-detect cases and post-treatment surveillance.
MANAGEMENT
Treatment involves surgery and chemoradiation. Early lesions may be treated with surgery alone whereas advanced ones may be treated by chemoradiation alone, as surgery would involve extensive resections with poor postoperative functional outcomes. Small superficial lesions confined to the tonsil-peroral monobloc are treated by tonsillectomy – securing adequate margins in all three dimensions.
Larger lesions require TORS (Trans Oral Robotic Surgery) or TLM (Transoral Laser Microsurgery) to include the underlying pharyngeal wall and/or the adjacent base of tongue to secure clear margins. Much larger lesions need a lower cheek flap approach with either a marginal or segmental mandibulotomy. TORS and TLM have comparable outcomes. They are advantageous because of less operating TORS and TLM have comparable outcomes. They are advantageous because of less operating time, lesser hospital stay, and improved swallowing outcomes post-surgery. Since the tissue is removed in pieces in TLM, histopathological examination becomes difficult and so it is less preferred. All cases undergoing elective surgery will also get their nodes removed, level II to IV. Both tonsils are removed, not the one with cancer alone.
Chemoradiotherapy is emerging as the treatment for choice for advanced tonsillar cancers as it preserves function. Radiotherapy with cisplatin chemotherapy is commonly used. Sometimes cetuximab is added when cisplatin is contraindicated.
PROGNOSIS
HPV-positive tumors have a significantly higher 5-year survival rate than HPV-negative tumors. HPV-positive tumors in smokers have a very poor prognosis.